|
|
| |
| |
Ventilation Systems in Operating Theatres,
Aspects to Consider
A JOHNSON MEDICAL BULLETIN (REPUBLISHED 2002)
by Agne Nilsson
1.0 Abstract
Ventilation is essential in all occupied premises. The requirements are determined by several factors such as fresh air supply for human habitation, control of airborne bacteria, thermal comfort, humidity level and so forth. The ventilation system is considered to be the main contributor to the function and efficiency of an operating theatre. It controls the level of comfort and the level of airborne contaminant, which often presents post-operative wound infection risks to the patients. Hence, the planning and designing of ventilation systems in operating theatres is crucial so that both infection rates and operating costs are lowered. This bulletin presents a summary of several conventional ventilation systems for operating theatres and a comparison among these conventional systems with the Johnson Medical Guided AirflowTM Ventilation System.
2.0 Introduction
A poorly functioning ventilation system in the operating theatres not only add unnecessary costs to healthcare facilities operating costs, it may also give rise to high infection rates and subsequent unnecessary sufferings to patients. Therefore, it has always been a complex task to plan and design an operating theatre that provides ergonomically good layout, ultra clean ventilation systems, low operating and installation costs. A lack of well-defined national and international standards on the overall function and ventilation standards of the operating theatre further complicates this task.
Currently available standards often place emphasis on the number of air changes and pressure relationships with adjacent areas. There are also standards on the particle concentration levels of different pollutants in the operating theatres. These standards, which have been produced, therefore only provide guide figures for occupational safety with the aim of reducing the risks of staff and patients being exposed to different pollutants or unpleasant odours. The main objective relates to selecting or designing a good ventilation system, which is capable of reducing post-operative wound infections, i.e. information not readily obtainable from standards.
3.0 Conventional Ventilation Systems for Operating Theatres
Various ventilation systems that have been designed and installed in operating theatres are largely classified into two main categories based on their respective operating principles. The two categories are mixing ventilation and parallel flow ventilation.
3.1. Mixing Ventilation
The mixing ventilation operates based on the principle that supply air mixes relatively rapidly with the existing air in the room. The supply air diffusion system is often located symmetrically on the ceiling. Published results on this type of ventilation system [1], [2] and [3] prove that the airflow is fairly unstable. The air is flowing in an uncontrolled manner and is subject to direction changes. Studies [1], [2] and [3] also show that during trace gas experiment, the area around the operating table has received trace gas concentration twice as high compared to other areas in the room. Therefore, in reality, the contaminant concentration level around the operating table will be twice as high. This in turn indicates the inefficiency of mxing ventilation and its inability to ventilate away anaesthetic gases and odours.
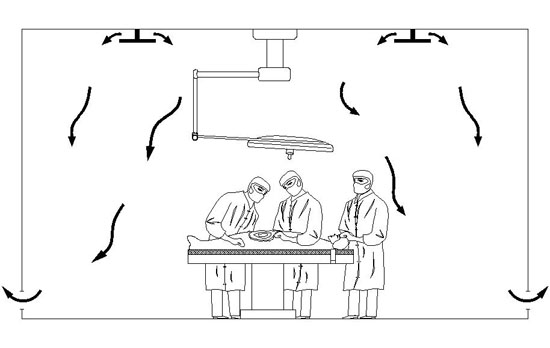 Figure 1: Mixing ventilation
Figure 1: Mixing ventilation
3.2. Parallel Flow Ventilation
The parallel flow ventilation operates based on the principle that supply air is conducted parallel through the room. The parallel flow ventilation systems can be horizontal or vertical flow. They have been used as conventional ventilation for operating theatres. Parallel flow ventilation is also commonly referred to as Laminar Air Flow system whereby the laminarity or uni-directionality of the air flow is said to exist in the operating theatre. H. Laufman from the Institute for Surgical Studies, Montefiore Hospital and Medical Centre, New York, once debated that laminar air flow cannot be achieved in an actively used operating theatre.
In 1982, it has been reported by E.A. Salvati, M.D., Journal of Joint and Bone Surgery, 1982, that horizontal parallel flow ventilation systems (Figure 2) are proven to be susceptible to contamination of the upstream air flow by the medical staff and surgical team with consequential increase in wound infection [14]. To reduce the risks, the only option is to build physical barriers, which would defeat the purpose for an ergonomic layout in the operating theatre. To further worsen situation, the horizontal supposedly uni-directional air flow would be disturbed by convection up-currents, thus generating turbulence and entrainment of contaminants.
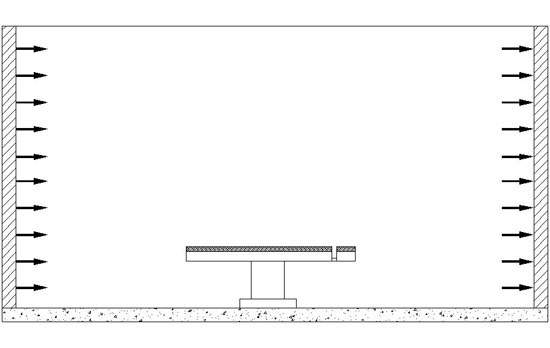 Figure 2: Horizontal Parallel Flow Ventilation
Figure 2: Horizontal Parallel Flow Ventilation
Vertical parallel flow ventilation (Figure 3) or commonly known as laminar air flow (LAF) system is a widely acceptable ventilation system used in hospitals and other heathcare facilities. These systems were very common in the sixties and seventies particularly for joint replacement surgeries. There are major drawbacks for this particular type of ventilation system. Both the installation and operating costs for this system are high. In order to achieve a low bacterial count (cfu/m3), LAF systems have to produce as high as 400 air changes per hour (ACH) [4]. Some LAF systems even produce up to 800 ACH. If the sedimentation processes for the room balance were disregarded and the inverse proportionality relationship between bacterial count and ACH is assumed, then a low bacterial count can only be achieved with the expense of high operating costs. LAF systems also commonly have 8-12 filters to cover the entire ceiling mounted diffusion system to ensure all the supply air is filtered before it enters the operating theatre. This has added unnecessary first costs during installation.
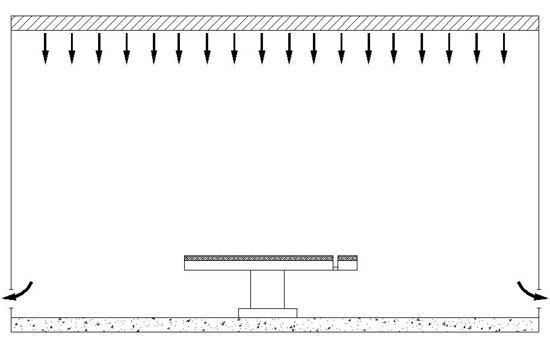 Figure 3: Vertical Parallel Flow Ventilation
Figure 3: Vertical Parallel Flow Ventilation
In 1960s and 1970s, Professor J. Charnley, UK, stated in his reports [5], [6] that the infection rate could be reduced from 7% to 0.5% by performing hip replacement surgery in an op-box ventilation system (Figure 4). However, all surgeons and medical staff had to wear tightly sealed surgical garments and masks with a special extraction system to achieve this result. Strict work discipline was also an influencing factor to prevent unnecessary vortex formation, which may convey bacteria to the sterile areas. These op-box systems have physical barriers such as curtains or wall systems built surrounding the surgical team. These systems therefore were popularly known as “op-boxes”. The major drawbacks for these systems are that surgeons suffered from poor mobility, poor visual contact because of misting on the hoods and poor communication through the hoods.
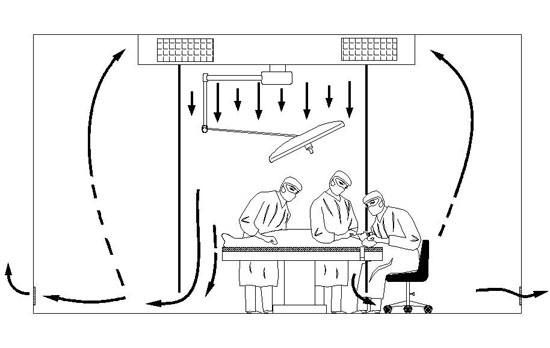 Figure 4: Op-box Ventilation
Figure 4: Op-box Ventilation
4.0 Johnson Medical Guided AirflowTM Ventilation Systems for Operating Theatres
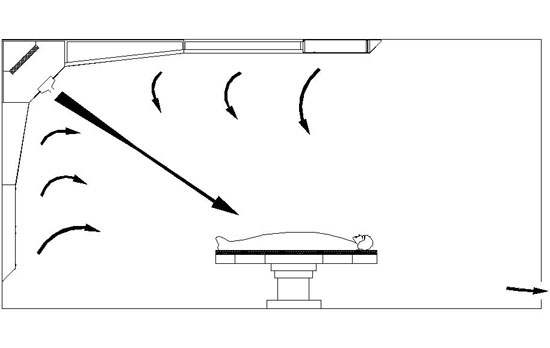 Figure 5: Johnson Medical Guided AirflowTM Ventilation System
Figure 5: Johnson Medical Guided AirflowTM Ventilation System
The Johnson Medical Guided AirflowTM Ventilation System (Figure 5) operates based on the principle that supply air is directed diagonally towards the operating table on the clean side of the room and exhausted out on the contaminated side of the room. The Johnson Medical Guided AirflowTM Ventilation System incorporates a slit ventilation, which has a booster-fed air jet. This newly developed slit ventilation system with the incorporation of booster-fed air jet is located at the intersecting area between the vertical wall and the horizontal ceiling on the clean side of the room. This ventilation system includes the provision of two large perforated supply air surfaces through which large quantities of sterile/fresh air feed into the co-ejection of the diagonal air jet in a controlled and stable manner. This system was developed in Sweden at the end of the eighties and has undergone thorough full-scale testing at the Royal Institute of Technology (KTH) and Royal Public Work Department. Full-scale clinical trials have also been conducted at the Swedish General Hospital, Ryhov Hospital, Jönköping with staff, equipment as well as various operating theatre arrangements. The tests and evaluations conducted by Professor C. Allander and Professor B. Ljungkvist at the Royal Institute of Technology, Stockholm, Sweden, have been appended in Appendix A at the end of this bulletin for clarity and reference.
A series of studies and experiments [1], [2], [3] and [7] conducted at the Department of Heat Technology, Royal Institute of Technology (KTH), concluded that among various air diffuser systems tested, the best results were obtained for the slit injection type ventilation. The air circulation at the operating table was proven to be stable independent of the activities carried out by the surgical team [8]. Most of the commonly used ventilation systems in operating theatres showed that the air flow pattern is unstable and disordered in both the operating and anaesthetic areas [8].
As a result of large supply air surfaces, the surgical instrument table is continuously flushed with sterile air (Figure 6).
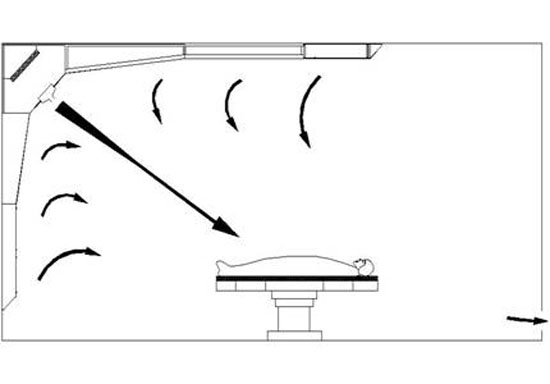 Figure 6: Sterile tables are continuously flushed with sterile air
Figure 6: Sterile tables are continuously flushed with sterile air
Bibliography & References
- Narkosgasspridning och narkosgaskoncentrationer inom sjukvĺrden. En orienterande ventilationsteknisk studie, institutionen för värmeteknik, KTH, 1980.
- Innala, Ö, Ljungquist, B. Ventilationsom förhindrar att föroreningar sprids, VVS 1:1982.
- Andersson, P.A., Hambraeus, A., Ljungvist, B., Neikter, K., Ramsjö, U., Zettersrtöm, U. A comparison between tracer gas and tracer particles techniques in evaluating the efficiency of ventilation. Journal of Hygiene, 1983.
- Mehta, Geeta. Microbiological surveillance of operation theatre. Orthoteers Orthopaedic Education Resource, Dec 2000.
- Charnley, J., Eftekhar, N.S. Postoperative infection in total prosthetic replacement arthroplasty to the bacterial contents of the air of the operating room. British Journal of Surgery 56, 641, 1969.
- Charnley, J. Postoperative infection after total hip replacement with special reference to air contamination in the operating room, Clinical Orthopaedics 87, 167, 1972.
- Ljungquist, B., öhlund, L. Operationsrumsventilation. En orienteering, Sjukhuset, nr 10, 1983.
- Ljungkvist, B., öhlund, L. Supply air system with slit injection for operating theatres. (Translated version of reference [16])
- Ljungkvist, B., öhlund, L. Luftspaltsystem med spalt inblĺsning för OP-salar. Tidskiften Sjukhuset4/86.
- Ljungquist, B., Hillerbrandt, B. Comparison between three air distribution systems for operating rooms. International Committee of Contamination Control Societies (ICCCS). 10th International Symposium on Contamination Control (ICCCS 90), Zurich, Switzerland, September 1990.
- Hemeon, W.C.L. Plant and process ventilation, Industrial Press, 1962.
- Nilsson, A. Operationskabiner. Planering avortopedoperationssal vid Eksjöklinikerna. Sjukhuset nr 5, 1983.
- Nilsson, A. Operationsboxar – infektionerock pĺverkande faktorer. Sjukhuset 7-8, 1983.
- Salvati, E.A., Robinson, R.P., Zeno, S.M., Koslin, B.L., Brause, B.D. and Wilson, P.D. Infection rates after 3175 total hip and total knee replacements performed with and without a horizontal unidirectional filtered air flow system. Journal of Bone and Joint Surgery 64-A, 1982, 525-535.
- Lidwell, O.M., Lowbury, E.J.L., Whyte, W., Blowers, R., Stanley, S.J., Lowe, D. Effect of ultraclean air in operating rooms on deep sepsis in the joint after total hip or knee replacement; a randomized study, British Medical Journal, July 1982.
- Ljungkvist, B., öhlund, L. Tilluftssystem med spalt-inblĺsning för operationssalar.
Appendix A
The following is a summary of the results for the tests and evaluations on different ventilation systems conducted by Professor C. Allander and Professor B. Ljungkvist at the Royal Institute of Technology, Stockholm, Sweden. The tests have been conducted using trace gas and smoke visualization methods as described by Allander and Ljungkvist. In most cases, these methods can be used to qualitatively investigate the operating theatre ventilation system with respect to particles of interest from a bacteriological point of view. A comparison between these ventilation systems and Johnson Medical Guided AirflowTM Ventilation System has also been included.
 Graph 1: Comparison of different ventilation systems vs. Johnson Medical Guided Airflow Ventilation System
Graph 1: Comparison of different ventilation systems vs. Johnson Medical Guided Airflow Ventilation System
Graph 1 depicts the CFU count for several ventilation systems under various conditions when tested in accordance to the standard test method as described by Allander and Ljungkvist. It clearly shows that normal ventilation systems can be easily affected by the level of activity in the operating theatre. The only systems that are capable of achieving consistent results are the Johnson Medical Guided AirflowTM Ventilation Systems and the Laminar Airflow (LAF) Systems.
To achieve such consistent results, the LAF systems require a massive airflow of 9000 m3/h, which resulted in high energy consumption and consequential high operating costs. Ljungqvist and Öhlund [9] also reported that the airflow rate for LAF systems have to be increased from a normal 2000 m3/h to 9000 m3/h to obtain a steady reading of 0.2 cfu/m3. These LAF systems are not only expensive to install, they are also expensive to run, maintain and often give rise to noise problems and a non-ideal working environment for medical staff.
In contrast, the Johnson Medical Guided AirflowTM Ventilation Systems are capable to achieve a bacteria count of 0.5 cfu/m3 with an exceptionally low airflow rate of 1800 m3/h. The results were obtained irrespective of the level of activity in the operating theatre. The Johnson Medical Guided AirflowTM Ventilation System is employing the slit injection technology, which has proven to be highly efficient. In 1990, Ljungquist and Hillerbrandt [10] presented in the International Symposium on Contamination Control, Zurich, Switzerland, that among all the air diffuser systems tested, the best results were obtained with the supply-air systems with slit injection. Better adaptation to the work routines of the operating theatre has also been achieved in the slit injection supply-air systems. One example of this is that the instrument-laying table is always flushed with sterile air from the air circulation point of view (Figure 6).
Note: CFU = Colony forming unit, is defined as a mass of bacteria which is the result of multiplication of one or more organisms. A colony may contain many millions of individual organisms and become macroscopic and its physical features are often characteristic of the species.
Agne Nilsson, Biomed. Eng., MTF, SFAI – Hospital and Research Engineer, Inventor
Agne Nilsson, originally from Sweden, is the Technical Director for Johnson Medical Technology (JMT). He is the founding member of the Swedish Society of Biomedical Engineering and Medical Physics. He also holds membership for the Scandinavian Society of Anaestesiologists and Swedish Society of Inventors. He is the author of the book ‘Medical Equipment Planning’.
Agne Nilsson works on hospital-related projects and has invented and designed a number of systems and medical equipment over the past 30 years. He was awarded the 1986 Development Stipendium by the National Development Foundation. He has extensive international experience on hospital planning. For the past 5 years, he has been working on providing functional and conceptual designs for different government and private projects and departments of hospitals in Malaysia.
|
|
|

